Dr Yvonne Shaw, Underwriting Policy Lead at Dental Protection, offers an overview of orthodontic claims received by members in the UK.
Dental Protection’s philosophy is to support safer practice in dentistry and to help members avoid problems arising in their professional practice. One of the many ways we look to support members in reducing risk is by sharing insights from our cases and claims to help understand how problems may arise and, most importantly, how they can be prevented in the first place.
As part of our ongoing commitment to share learning and insight from cases, Dental Protection has been developing systems to assist in the analysis of unstructured data contained within case files. One of the outputs of this work has been the production of a risk dashboard to support the identification of common themes in the cases we deal with. Further development of these analytical tools will enable us to identify themes and trends in cases more efficiently and, in turn, allow us to share more information with members about risks arising in different areas of practice. This is the first Dental Protection article to be produced that has used unstructured data analysis software to support the claims review.
A review of claims data was undertaken focusing on claims relating to orthodontic care that were opened at Dental Protection during the period 2016-2020. For the purposes of this article, the claims used in the analysis were those involving patients who were aged 18 or under at the time the first alleged failings in care arose. The claims reviewed related to treatment provided by both specialist orthodontists and non-specialist practitioners.
Out of the total claims identified in this data set, approximately 10% had allegations that related to root resorption. Of note, claims involving root resorption feature more strongly in our higher value orthodontic claims.
Root resorption claims
Root resorption is a recognised risk associated with orthodontic treatment, with potentially significant long-term consequences for the patient. It is, therefore, not surprising that a proportion of the higher value orthodontic claims we deal with will involve root resorption. In most of the child root resorption cases reviewed, common factors were noted, which may have made the patient at higher risk of teeth being affected by root resorption:
• Ectopic/unerupted canines (47%)
• History of trauma prior to commencing treatment (24%)
• Root shape (eg blunt root apices) (12%)
It should be noted that in the cases involving ectopic/unerupted canines, just over one third of the cases related to alleged delays in referral for orthodontic treatment. In these cases, root resorption had already occurred before any orthodontic treatment was considered or provided. The importance of monitoring the development and eruption of maxillary canines was the subject of a previous Dental Protection article
Ectopic canines – dentolegal challenges and how to avoid them.
Common themes in claims involving root resorption
As a recognised risk of orthodontic treatment, it is expected that patients for whom orthodontic treatment is being considered should routinely be made aware of the risk of root resorption as part of the consent process. It may therefore be surprising to see that in over 50% of the claims reviewed, alleged failings in the consent process were a dominant factor. Figure 1 below shows the main alleged failings in the claims reviewed.
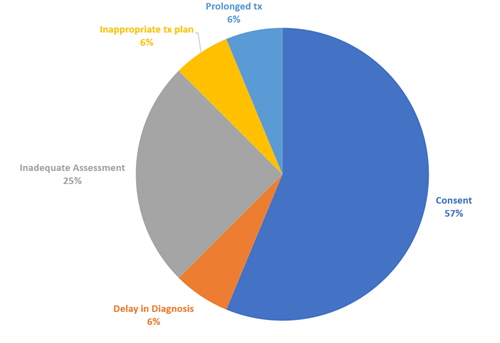 Fig 1. Common themes identified in child orthodontic claims involving root resorption – Dental Protection data 2016-2020
Fig 1. Common themes identified in child orthodontic claims involving root resorption – Dental Protection data 2016-2020
In many of the cases predisposing factors were present, which may have put the patient at greater risk of root resorption. To defend a claim of this nature, it would be important for the records to demonstrate that:
a) The increased risk had been identified
b) The specific risks that a particular patient faced had been discussed and understood by the patient
c) The treatment plan proposed was appropriate
d) Alternative ‘lower risk’ alternatives had been considered and communicated to the patient
e) Appropriate monitoring of teeth was undertaken during treatment.
Experts will invariably opine on the above and these are the points on which claims involving root resorption may succeed or fail. Where predisposing factors are present, and the records only provide evidence that a patient had been provided with generic information about the risks, it is unlikely the warnings will be found to be sufficient to demonstrate consent to treatment was valid. Where a patient is successful in their claim, damages can be significant. For a young patient, tooth loss may result in damages to cover a lifetime of implant placement and restoration cycles, as well as reflecting the psychological impact.
The issues displayed in Fig 1 were not the sole issues arising in the cases, with additional allegations relating to inadequate monitoring, prolonged treatment and poor outcome being the most common secondary factors. In around one third of the cases where predisposing factors were noted, secondary allegations were made that there had been inadequate monitoring of the teeth during active treatment. When considering these allegations, experts will comment on whether monitoring was in line with any recognised guidance and teaching. Where there is a lack of consensus, the case will be assessed on whether the approach taken was reasonable at that time. For those treating patients with a known history of trauma, guidance such as that recently published by Sandler et al
1 would be of relevance and may be relied upon by experts in future.
Allegations relating to consent, assessment and monitoring were common themes across both specialist and non-specialist practitioner groups.
Risk prevention
Orthodontic treatment is not without risk and for some patients the risks of treatment may outweigh the benefits. Ultimately the decision whether to proceed with orthodontic treatment rests with the patient, who must make this choice based upon balanced and objective information that has been shared by the treating clinician to help the patient understand the risks.
Identifying that significant root resorption has arisen is not only distressing for the patient, but also generates significant anxiety for the clinician who has treated the patient. It is, however, important to remember that this finding will not necessarily result in a patient making a complaint or claim, and they are less likely to do so if they had understood and accepted the risk of this arising at the outset.
Similarly, being the subject of a claim does not mean that the claim will need to be settled. In most of the cases we see, the successful defence of claims relating to root resorption will rely heavily on the details within the records, to demonstrate that the consent was valid and clinical treatment was appropriate.
As a general guide, the following checklist may help in the defence of a claim but, perhaps more importantly, avoid a patient going down this route in the first place:
• Ensure that any orthodontic assessment routinely includes an assessment of any potential risk factors for root resorption and documents both positive and negative findings.
• Where the assessment identifies a patient may be at a higher risk of root resorption, ensure that the records reflect the specific risk that patient faces and whether alternative treatment options, including no treatment at all, were discussed. Where risks are increased, ensure that any written information provided to the patient is tailored to reflect the identified increased risk.
• If it is proposed to monitor root health during treatment with radiographs, ensure that a clear note is made in the records as part of the treatment plan about when any radiographs should be taken. This is particularly important in settings where a patient may be seen by multiple clinicians or where care is being transferred.
• In the event root resorption is identified, it is important to be open and honest with patients and ensure that not only is the presence of the root resorption discussed but also what steps may be necessary to mitigate any further exacerbation of the problem. Before continuing with further treatment, the consent process should be revisited, and records updated to reflect the discussions and options discussed.
• In the event teeth are subject to trauma after treatment has commenced, ensure any assessment and ongoing treatment reflects contemporary guidance and teaching. It is important to also revisit the consent process to ensure the patient is involved in any further decision making and aware of the risks and alternative options.
1Cara Sandler, Tumadher Al-Musfir, Siobhan Barry, Mandeep Singh Duggal, Susan Kindelan, Jay Kindelan, Simon Littlewood, Hani Nazzal, Guidelines for the orthodontic management of the traumatised tooth, J Orthod. 2021 Mar;48(1):74-81.